See Page 12 of the Premier Academy Student Handbook for full uniform policy
Additional may be available at Premier Academy for $15 each Options:
- Portal Login
- Return to Learn / COVID-19 Plan
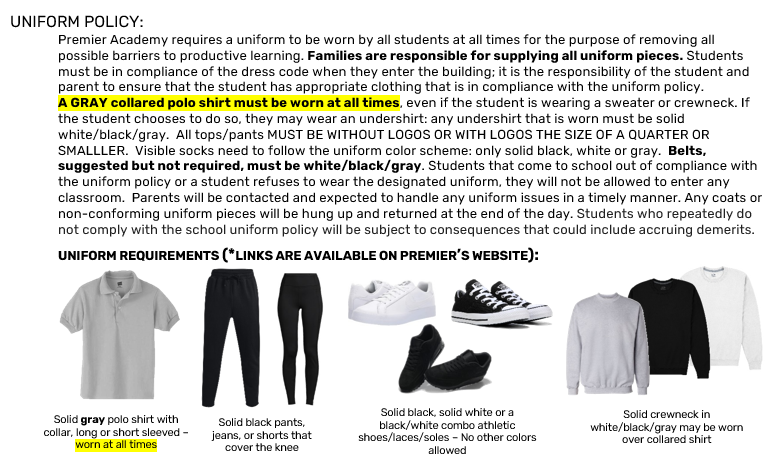
- Uniform Policy
- Polo Shirts
- Crewneck SweatshirtsSee Page 12 of the Premier Academy Student Handbook for full uniform policy
Additional may be available at Premier Academy for $15 each - Sweatpants SuggestionsSee Page 12 of the Premier Academy Student Handbook for full uniform policy
Solid black pants, jeans, or shorts that cover the knee (no holes, no logo) - Notes
- Truancy Policy